























Sitting is the New Smoking
Sedentary epidemicSitting and smoking: A comparative analysis Health consequences of sittingPromoting an active lifestyleReferencesFurther reading Sedentary behavior or insufficient physical activity can negatively impact an […]




Heres How You Can Maintain a Healthy Diet While Working From Home
Did you know that World Health Day is celebrated every 7th of April? Some people don’t even know that such a day exists! The 2020 health crisis […]




Having My Breasts Removed Helped Me Show My Daughters How To Be Comfortable in Their Own Skin
I wasn’t prepared for all the compliments I’d receive when I got my breast implants. I had perfect breasts. They were so ideal that I […]




Rift over when to use N95s puts health workers at risk again
Three years after more than 3,600 health workers died of COVID-19, occupational safety experts warn that those on the front lines may once again be […]



FDA Approves Zurzuvae
FDA Approves Zurzuvae (zuranolone) First Oral Treatment for Postpartum Depression August 04, 2023 — Today, the U.S. Food and Drug Administration approved Zurzuvae (zuranolone), the […]

FDA Approves Beyfortus
FDA Approves Beyfortus (nirsevimab) for the Prevention of RSV Lower Respiratory Tract Disease in Infants July 17, 2023 — AstraZeneca and Sanofi’s Beyfortus (nirsevimab) has […]

FDA Approves Veklury (remdesivir) for COVID-19 Treatment in Patients With Severe Renal Impairment, Including Those on Dialysis
FOSTER CITY, Calif.–(BUSINESS WIRE) July 14, 2023 — Gilead Sciences, Inc. (Nasdaq: GILD) today announced that the U.S. Food and Drug Administration (FDA) approved a […]

FDA Approves Yuflyma
FDA Approves Yuflyma (adalimumab-aaty), a Biosimilar to Humira JERSEY CITY, N.J.–(BUSINESS WIRE) May 24, 2023 –Celltrion USA today announced that the U.S. Food and Drug […]

KHN’s ‘What the Health?’: Wrapping Up Summer’s Health News
Can’t see the audio player? Click here to listen on Acast. You can also listen on Spotify, Apple Podcasts, Stitcher, Pocket Casts, or wherever you […]

‘Free’ Screening? Know Your Rights to Get No-Cost Care
An ounce of prevention … well, you know the rest. In medicine, prevention aims to spot problems before they worsen, affecting both a patient’s health […]








Rift over when to use N95s puts health workers at risk again
Three years after more than 3,600 health workers died of COVID-19, occupational safety experts warn that those on the front lines may once again be […]
Read moreClearing the cellular clutter: New insights into how our cells stay healthy
Reviewed If we don't take out the trash regularly, our homes become unpleasant and even a danger to our health. The same applies to our […]
Read moreLegal but not available: How powerful international banks are limiting accessibility of cannabis

A new study suggests that despite cannabis being legal in certain jurisdictions, such as Canada and Uruguay and 24 U.S. states, restrictions imposed by the […]
Read moreKey health department jobs dont exist, according to the federal government

Several key public health occupations are lacking a Standard Occupational Classification code (SOC), including disease intervention specialists, public health nurses, policy analysts, and program managers, […]
Read moreNight sweats reveal the severity of sleep apnea

In Greek, apnea (ἄπνοια) denotes the “absence of breathing.” Hence, obstructive sleep apnea is a disease defined by interruptions in breathing, which recurs while the […]
Read moreStudy reveals hidden inactive form of p38a protein
Reviewed p38a protein, a key enzyme in the regulation of various cellular functions, plays a crucial role in some diseases, including cancer, chronic inflammation, and […]
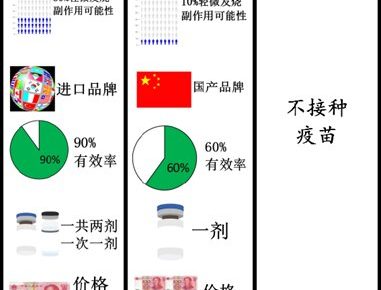
Read moreWhy isn't anyone allowed to pay for a Covid booster?

PROFESSOR ROB GALLOWAY: There’s a very good reason for us all to have a Covid booster. So why isn’t anyone allowed to pay for one? […]
Read moreQ&A: Why some California hospitals are still struggling after COVID-19

The COVID-19 pandemic hammered California hospitals by disrupting their operations and pounding their finances. Nearly four years after the onset of the pandemic, profit margins […]
Read moreQ&A: What sunscreen is best? A dermatologist offers advice on protecting your skin

Sunburn is a sign that skin has experienced significant levels of damage. Ultraviolet light can change a person’s DNA structure, which can lead to cancer. […]
Read moreTheres a black market on social media for pricey fertility drugs

After in vitro fertilization led to a miscarriage, Lindsay found herself with thousands of dollars’ worth of fertility drugs she could no longer use. She […]
Read more